

Basic Projections
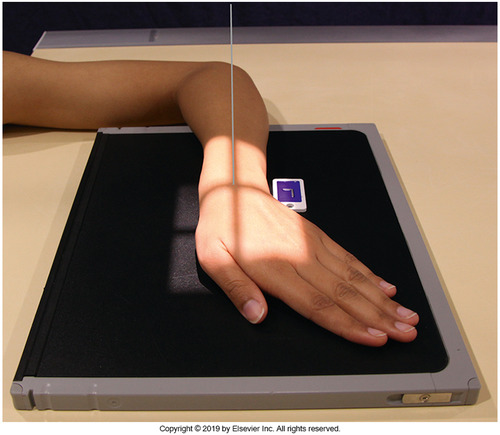
1. PA Wrist
- Purpose: Overview of distal radius/ulna, proximal metacarpals, and carpal alignment; screening for fractures and joint pathology.
- Positioning: Patient seated with shoulder–elbow–wrist in one plane; hand pronated; flex digits to bring carpals close to IR; palm flat on IR.
- Central Ray (CR): Perpendicular to midcarpal area.
- SID: 100 cm (40 inches).
- Collimation: Distal third of radius/ulna, all carpals, proximal third of metacarpals; ~1 cm skin margin.
- Anatomy Shown: Carpals with interspaces, distal radius/ulna, proximal metacarpals; radiocarpal and carpoulnar joints.
- Contraindications: If pronation not possible due to trauma or fixation, use AP wrist instead.
- Notes: Flexing the digits reduces OID of carpals and improves detail.
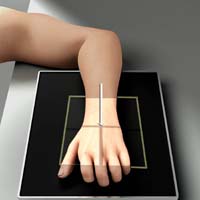
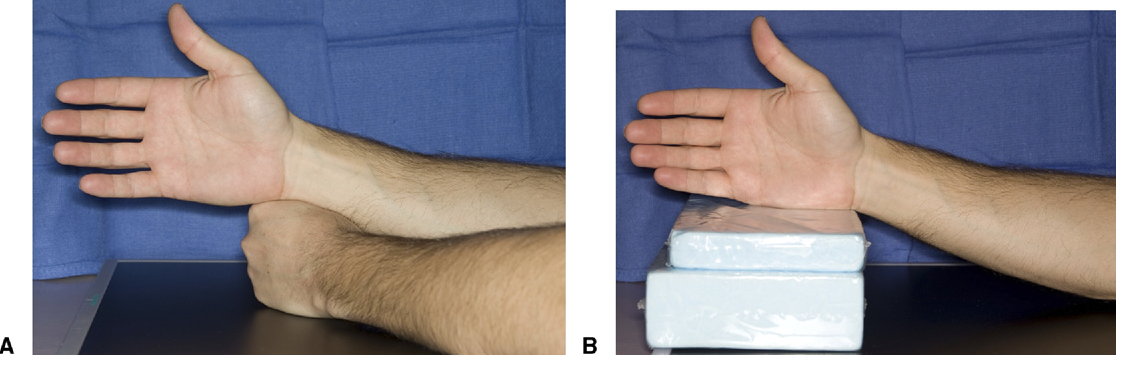
2. Lateral Wrist (Lateromedial)
- Purpose: Evaluate distal radius/ulna alignment, carpal dislocations (e.g., perilunate), and soft-tissue fat pads.
- Positioning: Elbow flexed 90°; wrist in true lateral (thumb up); shoulder–elbow–wrist in same plane; palm perpendicular to IR.
- Central Ray (CR): Perpendicular to midcarpal area.
- SID: 100 cm (40 inches).
- Collimation: Distal third of radius/ulna and all carpals.
- Anatomy Shown: Superimposed distal radius/ulna; lunate profile; assessment of scapholunate and radiocarpal alignment.
- Contraindications: If rotation is painful, pad/support to achieve lateral without forcing motion.
- Notes: Key view for Colles/Smith fractures and carpal dislocations; ensure true lateral to avoid overlap.
Additional / Special Projections
1. Scaphoid — PA with Ulnar Deviation
- Purpose: Elongation and isolation of the scaphoid to assess waist fractures and scapholunate interval.
- Positioning: From PA; deviate hand ulnarward as tolerated; forearm stays flat on table.
- Central Ray (CR): Perpendicular to scaphoid (anatomic snuffbox) or 10–15° proximally toward elbow if joint spaces are not open.
- SID: 100 cm.
- Collimation: Tight to scaphoid region; include adjacent carpals.
- Anatomy Shown: Scaphoid with minimal foreshortening; scapholunate joint.
- Contraindications: Avoid forced deviation in acute trauma—use Stecher instead.
- Notes: Mark “ulnar deviation” on image for clarity.
2. PA Clenched-Fist (Stress)

- Purpose: Dynamic assessment of scapholunate instability by stressing the SL ligament.
- Positioning: PA wrist; patient forms a firm fist or pulls against a radiolucent band.
- Central Ray (CR): Perpendicular to midcarpal area.
- SID: 100 cm.
- Collimation: As for PA.
- Anatomy Shown: Widening of scapholunate interval under load, if present.
- Contraindications: Avoid in acute scaphoid fracture or severe pain.
- Notes: Acquire non-stress PA for comparison.
3. Carpal Tunnel View (Tangential — Gaynor-Hart)

- Purpose: Visualization of carpal canal, hook of hamate, pisiform, and trapezium.
- Positioning: Forearm aligned with table; hyperextend wrist (dorsiflex) so palm approaches vertical; rotate hand slightly toward radial side.
- Central Ray (CR): 25–30° toward the palm (distal to proximal) to the base of the third metacarpal.
- SID: 100 cm.
- Collimation: Tight to carpal tunnel region.
- Anatomy Shown: Carpal canal with hook of hamate, pisiform in profile; trapezium and scaphoid tubercle.
- Contraindications: Do not hyperextend in acute trauma or suspected occult carpal fracture.
- Notes: Use gentle support to achieve extension; avoid patient strain.
4. Carpal Bridge (Dorsal Tangential)

- Purpose: Assessment of dorsal carpal pathology (e.g., triquetral avulsion “chip” fractures).
- Positioning: Dorsum of hand on IR; wrist markedly flexed (palmar surface near right angle to forearm).
- Central Ray (CR): 45° caudad (toward fingers) to a point ~4 cm proximal to wrist joint.
- SID: 100 cm.
- Collimation: Distal radius/ulna and all carpals.
- Anatomy Shown: Dorsal aspects of carpals; triquetral avulsions.
- Contraindications: Avoid forced flexion in acute trauma; consider PA and lateral alternatives.
- Notes: Pad under hand for comfort; maintain only tolerable flexion.
5. PA Oblique — Lateral Rotation (≈45°)

- Purpose: Demonstrates trapezium–first CMC joint and scaphoid waist with reduced superimposition.
- Positioning: From PA, rotate wrist/hand laterally 45°; support with sponge to maintain obliquity.
- Central Ray (CR): Perpendicular to midcarpal area.
- SID: 100 cm.
- Collimation: As for PA.
- Anatomy Shown: Trapezium and scaphoid in profile; open first CMC/trapeziotrapezoid joints.
- Contraindications: Avoid rotation if unstable distal radius/ulna fracture suspected; obtain PA and lateral first.
- Notes: Do not force rotation in trauma—use sponge.
6. PA Oblique — Medial Rotation (≈45°)

- Purpose: Better demonstration of pisiform, triquetrum, and hamate with less overlap.
- Positioning: From PA, rotate wrist medially ~45° (toward ulna); support with sponge.
- Central Ray (CR): Perpendicular to midcarpal area.
- SID: 100 cm.
- Collimation: As for PA.
- Anatomy Shown: Pisotriquetral joint and ulnar carpals more clearly visualized.
- Contraindications: Limit rotation if painful—prioritize PA and lateral.
- Notes: Useful adjunct for ulnar-sided wrist pain.
7. PA with Radial Deviation

- Purpose: Opens interspaces of ulnar-side carpals (lunate, triquetrum, hamate) and stresses TFCC region.
- Positioning: From PA, deviate hand radially as tolerated.
- Central Ray (CR): Perpendicular to midcarpal area.
- SID: 100 cm.
- Collimation: As for PA.
- Anatomy Shown: Ulnar carpals with reduced overlap; TFCC profile improved.
- Contraindications: Avoid forced deviation in acute trauma.
- Notes: Document degree of deviation if assessing instability.
8. AP Wrist (Alternate for Limited Pronation)

- Purpose: Alternative overview when pronation is not possible; demonstrates carpal interspaces differently from PA.
- Positioning: Forearm supinated (palm up); posterior wrist on IR; digits relaxed/slightly flexed.
- Central Ray (CR): Perpendicular to midcarpal area.
- SID: 100 cm.
- Collimation: As for PA.
- Anatomy Shown: Carpal interspaces more open anteriorly; distal radius/ulna.
- Contraindications: Prefer PA when feasible; AP mainly for non-pronating patients.
- Notes: Avoid tight finger flexion that might rotate the forearm.
General Notes
- Remove jewelry and metallic objects.
- Align shoulder–elbow–wrist in the same plane to prevent distortion.
- In trauma, prioritize non-manipulative views (PA and lateral) before stress or deviation views.
- Consider additional forearm or dedicated hand views if clinical suspicion extends beyond the wrist.